Blog, News & Views




Our Ski Fit Series- Ski Posture
https://www.facebook.com/boostphysio.hendon/videos/2038905709459180/








10 Tips and Facts About Knee Pain

Tosin has been solving patients knee pain for more than 14 years!
 Ronnie has been doing it for over 20 years!
Ronnie has been doing it for over 20 years!









The most common mistake made when exercising is doing too much too soon- often causing injury.
Here are our 5 tips to ensure you progress exercising safely.
- Progress cardio exercise by no more than 10% per week. This gives your muscle and joint tissue time to adapt. You will feel able to do more, hold yourself back and progress slowly.
- Don’t try and compete (too much) with the person next you in the gym or exercise class- ego can often be one of the major causes of sports injury!
- Listen to your body- delayed onset muscle soreness (DOMS) for a few days after heavy or new exercise is normal, but if this is muscle ache is lingering or getting worse- back off and listen to your body.
- Give your body adequate rest and recovery enabling microscopic tissue damage to repair. Having 1-2 rest days per week is always recommended.
- It is impossible to perform at 100% every workout- Usain Bolt cannot run a world record every single race.

The feet are made up of 26 bones and 33 joints and carry people around for thousands of steps every day. So it is no surprise that foot pain is very common.
The great news is that foot pain is very treatable and there is plenty you can do yourself!
Here are 5 great exercises that can be done to help treat and manage foot pain. These were created by the Chartered Society of Physiotherapists for Arthritis Research UK.

7 Things Runners Must Know
Your shoes – if you are new to running go to a specialist running shop for an assessment and advice on which shoes are best for you. A bad pair of trainers can lead to blisters, knee pain and conditions like plantar fasciitis. “Under no circumstances should you ever wear new running shoes for the first time for a race”, says Tosin.
Get a check-up and a tune up – if you were taking your car on a long cross country journey you’d get it checked out before you left. The same for your body. Even though you are probably pretty fit it is worth taking some professional advice. Ask a specialist physiotherapist to carry out a biomechanical assessment to pinpoint any issues that need tweaking.

Stretch and stretch again – Stretching is an important part to your training schedule for injury prevention. Dynamic stretching is advised pre-run and a mixture of dynamic and static stretching is advised post run. The use of a foam roller can be a great tool and a regular sports massage will provide benefit and reduce the risk of injury.
Don’t ramp up your training too soon – Remember to progress your mileage sensibly, especially on your longer runs. A quick and high jump in mileage can lead to calf strains and cartilage issues in the knee. “Stick to the plan and don’t push onto the next goal before you need to. If you feel like you can do more that’s a good sign”, says Tyrone.
Sleep – make sure you get enough sleep, your body needs to repair and those early morning pre-work runs can take their toll if you are not sleeping enough.
Training injuries – Seek advice a specialist physiotherapist who will be able to get accurate diagnosis or a precise diagnosis who will treat and basically how quickly you can get back to training.
Sports massage – make sure you have regular massages and book one for after the event, you’ll be very glad you did.

Running on an empty stomach – It is never a good idea to run without fuel. If you are not fuelled up you will get tired a lot quicker and possibly cause damage to muscle because you are burning muscle. A sensible marathon diet can and will make all the difference to your training.
A word about socks – just like trainers, you should never wear new socks for the actual event as this can lead to blisters. Like your running shoes, make sure you’ve done at least one or two long runs in the socks and trainers you intend to wear for the marathon.
Our 5 Tips to Avoid Tech-Neck featured in Reader’s Digest Magazine

Adjust your car seat to avoid back pain





Back Pain Myth Busters- we’re busting myths and reinforcing what the latest evidence says is best for your back.




Triathlon season is in full swing, many of our patients are preparing for their first triathlon at the London Triathlon in August, which is one of the biggest triathlon events in the world.
Steven Berkman who has completed 5 triathlons and owner of BOOST PHYSIO, explains 4 things every first time triathlete “Must know”. This article was published by Oh My Quad Fitness Magazine

80% of injuries occur in training and problems can arise when you put yourself on a rigorous training schedule. You are probably fitting in your triathlon training with your work life, commute and commitments at home and it’s easy to get obsessed and keep training without proper recovery time to ensure you stay on schedule and unfortunately that is when you can get injured.
1) Is it an injury or aching muscles?
You’ve set yourself an incredible task of training for a 1.5k swim 40k cycle and a 10k run. It is inevitable that you’ll feel some aches and pain after exercising regularly.
Problems start, especially for first time triathletes, when you keep training through the pain and it doesn’t get better after a few days. Knowing when to stop, what the signs of injury are can be key to a successful triathlon experience.
The main injuries people suffer from when training for a triathlon are usually shoulder pain from swimming, cycling injuries are usually knee or hip related and running are usually from the knee down to the foot area.
Hopefully the pain you are experiencing is DOMS (Delayed Onset Muscle Soreness) and not pain from injury. Athletes and fitness know their workout is working when they have DOMS and if you start your triathlon training with a reasonable base of fitness you will expect the pain and achiness that comes 24 to 48 hours after heavy exertion. DOMS is normal and is often a gratifying feeling after having pushed yourself, it usually improves after a few days.
If it is DOMS you will feel better after an easy cycle or jog but an injury will make the pain worse and that is when you should seek professional advice. Look out for pain or swelling around the knee or ankle, localised soreness or areas that are painful to the touch. If your pain is interfering with your daily routine, climbing the stairs, getting out of your chair or out of the car, if you knee is locked or if a hip or ankle feels stiff and painful then chances are it is an injury.
If the pain impedes your training, say you usually cycle for 80 minutes but you can’t do more than half an hour then it’s more likely to be an injury.
2) Don’t panic
If you do get injured during triathlon training don’t panic. It doesn’t mean you can’t take part in the event. Depending on the severity of the injury and the amount of time left before the triathlon a good physiotherapist should be able to help you get back to training so you can compete in the event.
3) Make sure you do enough Brick Training Sessions
A Brick training session is combining to of the events into one training session. For example a swim followed immediately by a cycle, or a cycle followed immediately by a run, rather than keeping your training regime separate all the time. The point is to practise what it feels like to have jelly legs when you get off the bike or how to stop getting dizzy when you get out of the water after a long swim.
You need to know what it feels like so you know how to put the least amount of stress on your body when you transition between activities. It is tempting for a newbie to rush between activities at the main event in order to save time but the key here is slow and steady.
4) How to transition safely during training and at the main event
Simply knowing what is happening to your body as you go through the transitions at the triathlon will stop you worrying or panicking that something is seriously wrong, forewarned is forearmed and it is reassuring to know that what you are experiencing is normal.
Transition 1: Swim to Cycle – how to avoid post-swim dizziness
It is not unusual to feel dizzy after you’ve been horizontal for half an hour, the blood drains from your brain and you may get wobbly knees, when you come out of the swim into Transition 1. Take your time coming out of the water, don’t try run straight away , rather walk quickly- do lots of deep breathing and pump your leg muscles to get blood to your brain while you adjust to being vertical. Practice in the pool, do twenty lengths, stand up, and walk around to get used to the feeling from going from horizontal to straight.
Transition 2: From Cycle to Run – how to avoid jelly legs
Make sure that you spend the last five minutes of the bike ride spinning at a higher cadence which will start loosening up your legs in preparation for running. While this sounds counterintuitive, slow down towards the end of the cycling section. It will be very tempting to go for one last hard push but most novices will benefit by preparing their legs before they start running. The key tip here is walking not running immediately after getting off your bike, you will not lose any significant amount of time and walking through Transition 2 will give you’re your body time to adjust in preparation for the 10k run.
When you start running you’ll have jelly legs so start with shorter paces, and spend the first five minutes lengthening your stride and start speeding up as your muscles start to adapt from cycling.
Sometimes it is worth checking in with a physio if you have any concerns and don’t forget to book a sports massage for after the big day.
Hopefully these tips will help first-time triathletes feel confident and prepared for what lies ahead for the big adventure that is taking part in a triathlon.
Pain problem that is not going away? Physiotherapy or Surgery not helped your painful condition fully? Read more about the role of a pain management specialist.
Jolene Sher, from BOOST PHYSIO Hendon, asks Consultant in Interventional Spine & Pain Medicine, Dr Nigel Kellow key questions about Pain Management.
Dr Nigel Kellow MB BS FRCA is a leading specialist in painful spinal, skeletal, and neurological problems and one of his main areas of interest is the use of percutaneous image guided procedures.
Dr Kellow practices privately in London and you can find out more about his practice on his website here: www.kellow.com
1) When is the right time to see a pain management consultant?
A. Pain specialists deal with problems that a) have been caused by surgery, b) can’t be treated by surgery, or c) for which surgery is not indicated. So I see a lot of surgical complications, e.g. .nerve injuries, prolonged or severe postoperative pain delaying recovery or impairing function. I see CRPS whether related to surgery or trauma. I also see patients who are trying to avoid spinal surgery, for whom it isn’t indicated, or where they have continuing pain in spite of, or because of, spinal surgery. In practice this means a lot of patients with back and neck pain, sciatica or brachalgia, of all ages. The right time to refer to a pain specialist is as soon as any of these criteria have been met. With respect to the patients you see it will be anyone with sciatica or brachalgia whose pain is not well controlled; anyone who is not responding to treatment for back or neck pain; anyone with a possible serious problem; anyone for whom you want imaging; anyone with CRPS; anyone who has recently had surgery, whose physio is being impaired by inadequate pain control.
2) What treatments do you offer as a pain management consultant?
A. Triage and diagnostics – Full clinical and diagnostics assessment with advanced medical imaging (MRI, 3D CT, SPECT-CT), bone densitometry, neurophysiology, blood chemistry.
Treatment – medications (eg. anti-nociceptive drugs, anti-neuropathic drugs, muscle relaxants, opioids if necessary), spinal injections, nerve ablation, tumour ablation, spinal cord stimulation.
3) You deal a lot with spinal cord stimulation. What is this?
A. This is the implantation of electrodes and a pulse generator into the spine. Common indications include FBSS (Failed Back Surgery Syndrome – persistent pain in the back or legs after spinal surgery), CRPS, neuropathic pain. See this link.
4) What is the role of Physio in pain management in your opinion?
A. It plays an essential role throughout the spectrum of care of the patient in pain. Patients in pain always suffer from impaired function. It is vital that physios and pain specialists collaborate so I can make sure the patient’s pain has been adequately controlled so you can do your job as effectively as the patient’s MSK system will permit – whether this is following an acute injury, or after surgery.
After I have treated patients it is vital that they have physio during the window of opportunity afforded by any treatment I have done for them.
5 Reasons why your Health Insurance is not as good as you thought it was
Having worked as a physiotherapist for 19 years with all different health insurance companies, here are my top 5 insights why your insurance might not be as good as you thought it was…

- You paid for a Mercedes, what you got was an old banger! “I work in the city, my company provides the best corporate health insurance around- I can see who I like”… possibly not! You will find that more and more Consultants, Surgeons, Anaesthetists, Physiotherapists and Osteopaths are choosing to no longer deal with certain insurance companies. Most insurance companies won’t even contribute their normal “cheaper” rate towards you seeing the specialist who you want to see, that is not on their list.
- “Health Care Adviser” in a call centre calls the shots. You ring your health insurance claim hotline and after some brief questions and discussion on the phone the “adviser” in the call centre decides what you can and cannot have done. The expert view of your GP, Consultant or Physiotherapist whom you’ve seen and built a relationship of trust with, holds little sway over what the call centre decides they will or will not cover you for.
- “The Computer says No”. You manage to get the desired test or treatment authorised by the call centre. You feel a sigh of relief, but the relief is short-lived as the adviser says “this specialist is not on our list, but we can send you to someone else”. Your Consultant or Physio recommended you to a particular doctor or specialist, because they thought carefully about matching you with the specialist who has the best expertise, bed-side manner and availability for your condition. The call centre then provides you with an option that is in the insurance company’s best interest, not in your best medical interest…the call centre have never even met you! It usually feels like a bonus nowadays if the consultant you wish to see is on your insurance companies list. Always push the company to let you see whom you’ve been recommended to see.
- 4 Treatments or less! Did you know that 3 of the biggest health insurance companies expects your physiotherapist to see you for 4 treatments or less (one company only authorises 3 treatments)? Insurance companies are holding physiotherapists and consultants to sessional averages, threatening de-registration should the physio or consultant not work within the limit set by the insurance company.
- Your Policy says you have xxxx Pounds of Physiotherapy available, but the call centre only allows you £250. This is one of the cheekiest things… you bought your policy knowing that there was let’s say a £1,000 limit for physio, yet the insurance company will determine how much of it you can spend, that £1,000 limit could in fact be £250 or less.
Read what client reviews have said on TRUSTPILOT, an independent review website here…
More customer reviews about major health insurance companies here…
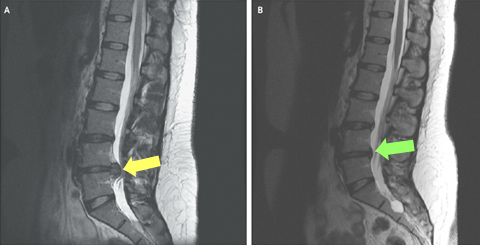
MRI of a lumbar spine showing slipped disc before and after treatment
What is a Slipped Disc?
The above scan belongs to a 29 year old woman who presented with new-onset pain and tingling in her right leg. The patient had a steroid injection, as well as a course of physiotherapy including soft tissue work, stretches and core strengthening. Within five months, her disc herniation had resolved, the pain and paraesthesia had completely gone. (Hong, J & Ball, P (2016) N Engl J Med 2016; 374:1564)
Figure A: MRI at the time of injury; the yellow arrow shows a lumbar disc herniation and nerve root compression.
Figure B: MRI at 5 months post-injury; the green arrow shows the disc is no longer compressing the nerve or spinal cord (white/grey column next to the vertebrae), with complete resolution of the slipped disc.
What is a slipped disc?
The spine is made up of 24 vertebrae that are stacked on top of each other. Between each vertebra, there is a disc made of a soft gel-like material, which acts as a shock-absorber or cushion. Discs are vital to help your back maintain its flexibility and range of movement. A slipped disc is a very common cause of back pain, and although the name can sound quite dramatic , it can be reassuring to note that the disc doesn’t actually ‘slip’.

The red area shows the leaked disc fluid pressing on the spinal nerve (yellow), which can become inflamed, causing back pain and symptoms down the leg.
The outer-shell of the disc becomes damaged, so the gel inside protrudes, also known as a herniation. The discs lie directly adjacent to the spinal nerve root, therefore the leaked disc fluid puts a lot of pressure directly onto the nerve, causing back pain. When the nerve is compressed or irritated, the symptoms can spread down your legs causing numbness, tingling or weakness, called a radiculopathy. In many people, the sciatic nerve is affected, resulting in sciatica or neural symptoms down the leg. A slipped, herniated and bulged disc all essentially refer to the same type of injury. The variation in name can indicate how much of the disc fluid has leaked out, and whether or not it is compressing the nerve.
What causes a slipped disc?
With age, the discs lose some of their water content, making the disc less effective as a cushion, and more susceptible to injury following minimal strain or effort. Sometimes twisting or turning whilst lifting heavy objects can lead to a slipped disc, and people often don’t realise the extent of the injury at the time. The disc can put pressure on either the whole spinal cord or just a single nerve root. This means that you can have pain in the back where the herniation occurred, or other areas of the body that the affected nerve controls, for example the buttocks or feet.
How do you treat a slipped disc?
There are different options for management. In many cases, the pain will go away on its own, as the disc eventually shrinks away from the nerve, reducing the pressure on the nerve and relieving the pain on the affected nerve. This can take 6-8 weeks, or sometimes longer. Having a course of physiotherapy can usually help to relieve the pain, tightness and inflammation around the lumbar spine and associated muscles. Physiotherapy treatment often uses a combination of techniques to speed up healing, reduce pain, increase flexibility and strengthen the surrounding muscles. Core stability exercises or Pilates can help strengthen the back further and reduce the risk disc injuries recurring in the future. In more severe cases, an Orthopaedic Surgeon can be consulted who will usually do a scan to determine whether procedures such as steroid injections or surgery are required.
If you suspect a slipped disc, try to keep doing gentle movements and activities as much as possible. You make need to take pain killers and rest from the aggravating factors, but try to keep moving as much as you can to prevent further tightness and stiffening.
If you have a slipped disc, or would like to speak to us about treatment options, and physio for your back pain, please call us on 0207 7949078 or book online.

Written by Naomi Sofer, Senior Physiotherapist
“It has been extremely rewarding getting Dr Maxwell (87 years old) back to playing tennis twice a week, after 5 sessions of physio” says our team.
Dr Maxwell is a regular at her local tennis club, playing doubles twice a week. Dr Maxwell, a retired Doctor, had a sudden flair up of hip and knee joint pain in February 2016, after playing a longer session of tennis. The pain was so great it caused Dr Maxwell to walk with 2 sticks and caused her immense pain.
After 5 visits over 4.5weeks we were able to help get Dr Maxwell back onto the tennis court! It is always much easier helping someone recover following injury when they are motivated and start from a point of fitness. Importantly Dr Maxwell always wants self-treatment methods and exercises that she can do to help herself recover.
Hampstead Physiotherapy Practice asks Dr Maxwell what the secret to her longevity is:
1) HPP: Playing tennis twice a week in your 80s- what’s the secret?
Dr Maxwell: I have played tennis since I was at school and am determined to continue as long as possible. I love the game. My running is limited now but I can still control the ball quite well and I have very tolerant partners. At 87 I still get an enormous amount of pleasure from playing, both physical and social. I hope my partners feels the same!
2) HPP: People with osteoarthritis are often afraid that sport and exercise will wear out their joints more quickly and worsen their condition. What is your experience in this regard?
Dr Maxwell: I believe regular exercise without too much strain can only be beneficial.
3) HPP: What do you do when you do have an injury, to help you get back onto the tennis court?
Dr Maxwell: I seek professional advice and as soon as I am fairly pain free and sometimes even before, I re-start specific exercises and general exercise. I also find ultrasound treatment can be very helpful.
4) HPP: How important have the rehab exercises prescribed by physios been in your various injuries?
Dr Maxwell: The rehab from physio has been an enormous help. In particular dealing with a torn achilles tendon and a dodgy knee in the past. I try to do a programme of general exercise (about 10-15min) every day and a specific one for tennis before I play.
If you have a tennis injury and would like an expert opinion on recovery please get in touch with us at The Hampstead Physiotherapy Practice, NW3. We often have same day appointments available. Why wait? Why wonder?
Is sitting really so bad for me? Or is sitting the new smoking?
Sitting is probably even worse for you than you think. Are you reading this sitting down? Do you spend most of your day sitting at work, sitting in the car, on the train? For years we have known that sitting stresses the joints and discs of the spine enormously. There is a strong link between sitting and back ache. Now over the past few years a growing group of Scientists and Doctors is calling sitting the new smoking. Not only bad for your spine, but bad for your health too.
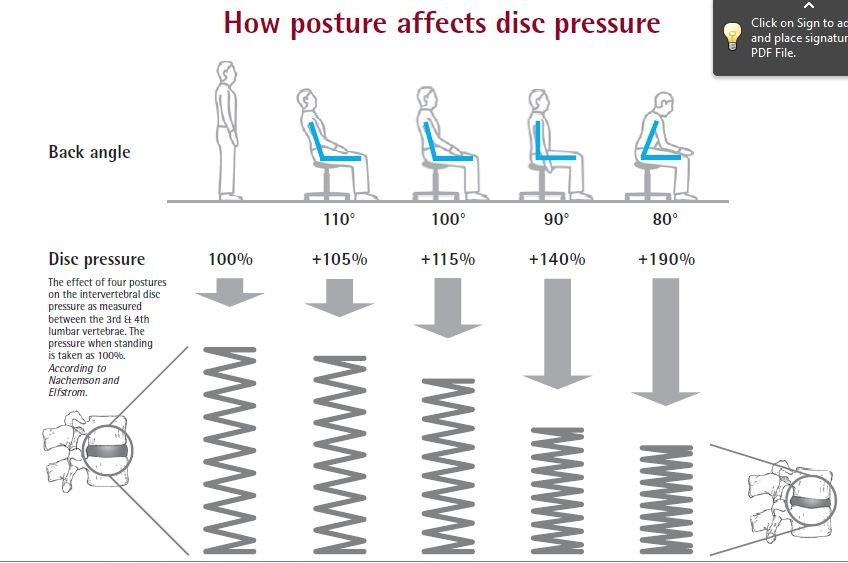
First let us look at the impact of sitting on the spine and posture, then we will explore why sitting has such a negative impact on health overall. Sitting loads the joints, muscles and discs in the lower back. Compared to standing, sitting, even with good posture, increases the pressure in the discs of the spine by 40%. Sitting with bad posture sees this disc pressure 90% more than standing.
Accumulative pressure over hours and days causes micro-trauma to the cartilage rings surrounding the outside of the disc, called the annulus. Over time the annulus rings can develop tears, weakening the disc and making it vulnerable to a more serious issue- bulging of the disc. A disc bulge happens usually when bending down, or lifting something, when the nucleus pulposus (the jelly like centre of the disc) squeezes through the torn rings of cartilage of the annulus. This is often called incorrectly “slipped disc”, but discs do not “slip”, they bulge.
This bulging disc can be very painful in the lower back and even more troublesome if it touches a nerve exiting the spine. When one of these nerve roots gets compressed or irritated by the disc, it causes a shooting pain in the leg, sometimes even tingling or numbness- this is often called sciatica.
7 Steps to reduce back strain from sitting:
- Stand more, sit less.
- Stand up at least every 45minutes.
- Sit up tall like a soldier, do not slouch.
- Avoid low, soft sofas.
- Maintain the arch in the low back with a rolled up towel.
- When learning stand at a shtender.
- Make a “standing desk” for work.
We can appreciate the negative impact of sitting on our spine and posture, but is sitting really so bad for our general health? Do you know that the Department of Health in England recommends adults have moderate exercise of at least 30minutes, 5 times a week. Moderate exercise could be brisk walking, cycling, swimming, gardening, gym etc.
An Australlian diabetes research study coined the phrase “Active Couch Potato”. This referred to people who did moderate exercise for the recommended total of 150minutes per week, but were mainly sitting the rest of the day. Among these “Active Couch Potatoes” they found negative effects to blood pressure, cholesterol, blood sugar and other readings. In other words, being sedentary all week continues to have negative health effects, even if one is doing moderate exercise 5 times a week.
The body is a moving machine that functions best when it is moving regularly. Studies have shown that children who are taught standing up, rather than sitting down can score better in exams. It seems even the brain might function better when the body is more active.
Move more and sit less with these steps:
- Walk rather than use the car.
- Take the stairs rather than the lift.
- Get off the bus or tube 1 stop earlier and walk the rest.
- Stand on the bus or tube for some of the way.
- Stand up when talking on the phone.
Our private physiotherapy clinics treat patients from all over North West London and North London. We provide same day physiotherapy treatment for sports injuries, neck and back pain.
Patients come for physiotherapy from the following areas: Hendon NW4, Mill Hill NW7, Cricklewood NW2, Hampstead NW3, Kilburn NW6, Queens Park, Finchley Road, Golders Green NW11, Swiss Cottage and Willesden Green NW10. Fortis Green, Muswell Hill, Highgate N6.
If you do have nay issues that need attention please book an appointment at one of our 4 High Street Physiotherapy clinics.
Physiotherapy hendon, hendon physiotherapy, physio cricklewood, cricklewood physio, physio NW2, NW2 Physiotherapy, Physio N6, Highgate Physio, physiotherapy highgate, physio hendon, hendon physio, physio nw London, nw London physiotherapy
What is the best position to sleep in?
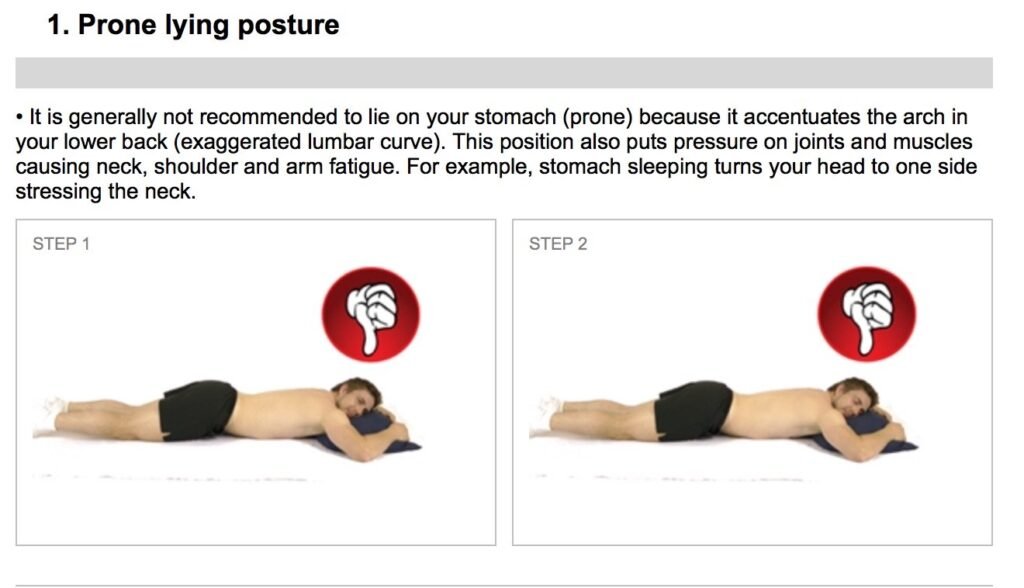
Sleeping on the tummy can strain the neck and the lower back
- On your back?
- Is sleeping on your tummy bad?
- How many pillows should be used?
- If my neck hurts how should I sleep?
- What’s the best position to sleep in with back pain?
Which position is best to sleep in?
We spend 6 to 8 hours a day sleeping, time that is essential for the body’s recovery, repair and growth. Most of us have also awoken with a sore back or a stiff neck from sleeping awkwardly.
The most comfortable sleep position, mattress and pillow arrangement will be whatever enables the body to remain in a neutral, compression free, middle range position for most of its joints. Joints held at either extreme end of their range of movement for a length of time can become painful and irritated by this sustained position.
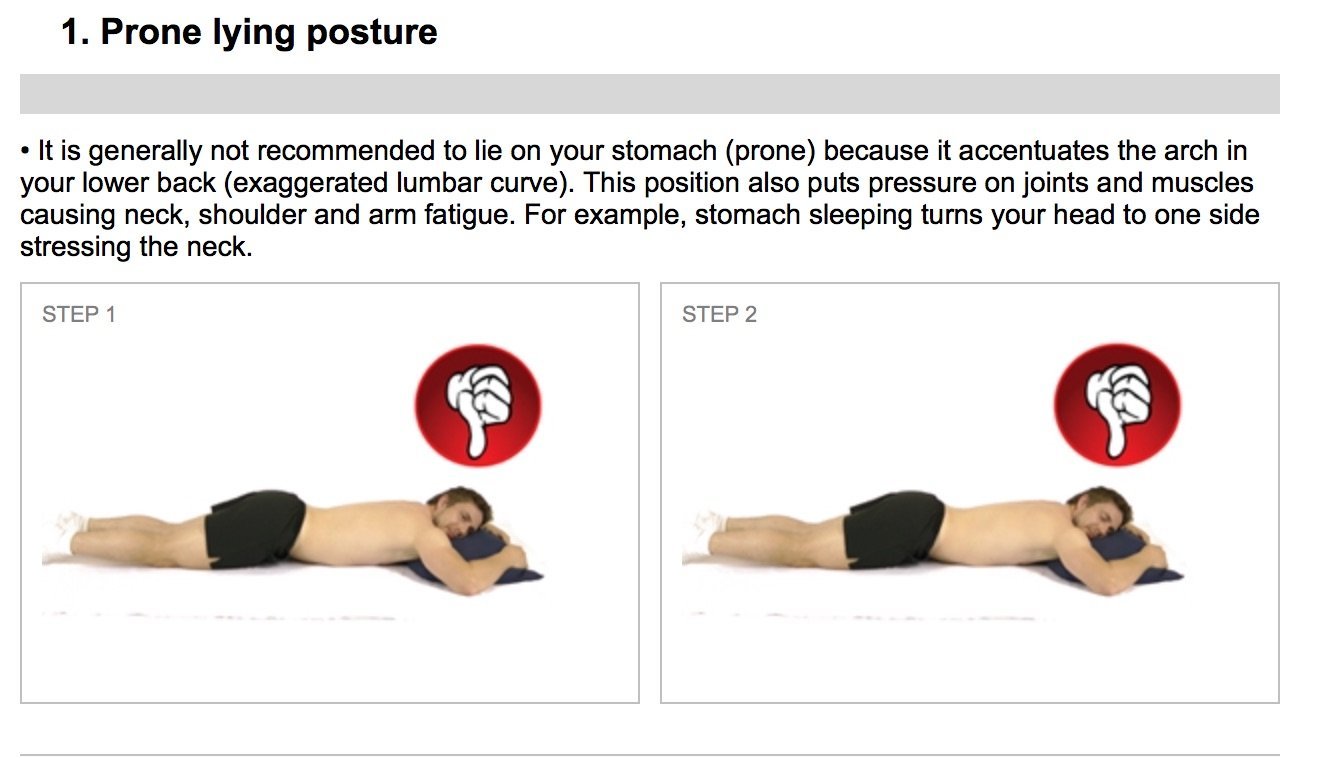
1) What is the best position for sleeping at night? The worst position is sleeping on the tummy. The neck is always twisted in one direction for most of the night causing uneven pressure on the cervical vertebral joints in the neck. There is also unbalanced tension in the muscles of the neck. Spending hours lying on the front can also cause compression of the facet joints, small joints on the back of the vertebra, causing back ache.
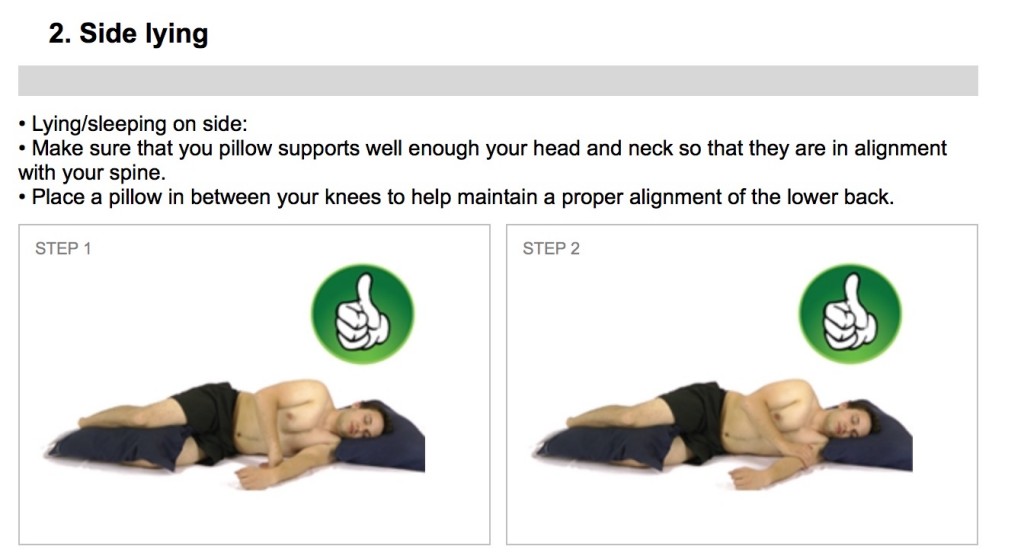
For most people sleeping on the side is ideal. The knees and hips should be slightly bent up with a small pillow between the knees. This small pillow between the knees reduces pressure points building up between the bony insides of the knees. This pillow has the added advantage of preventing the pelvis from falling forwards rotating the lumbar spine. Many with shoulder pain or hip pain find sleeping on the painful side to be difficult as there is hours of pressure on the painful area, which can be very uncomfortable.
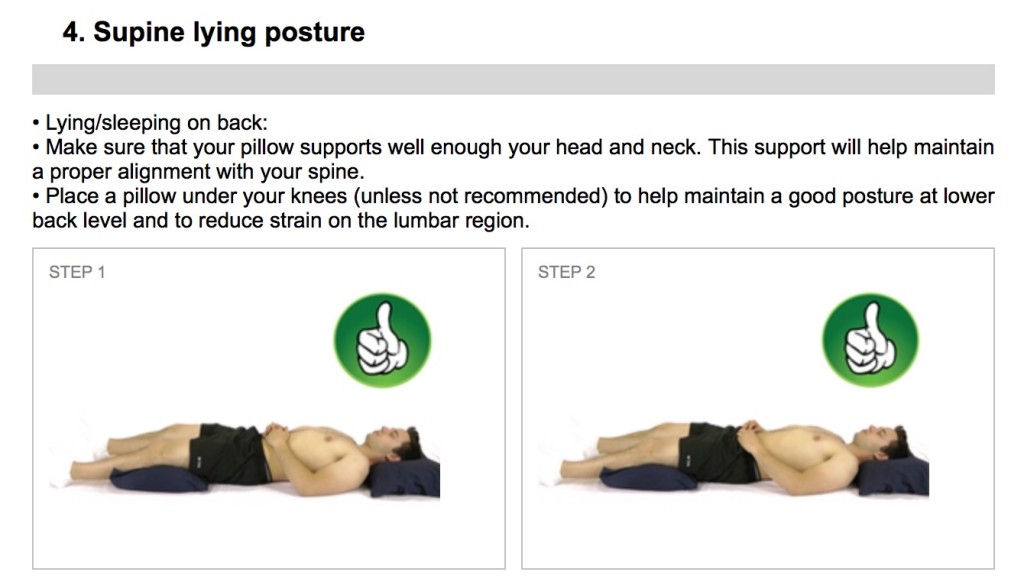
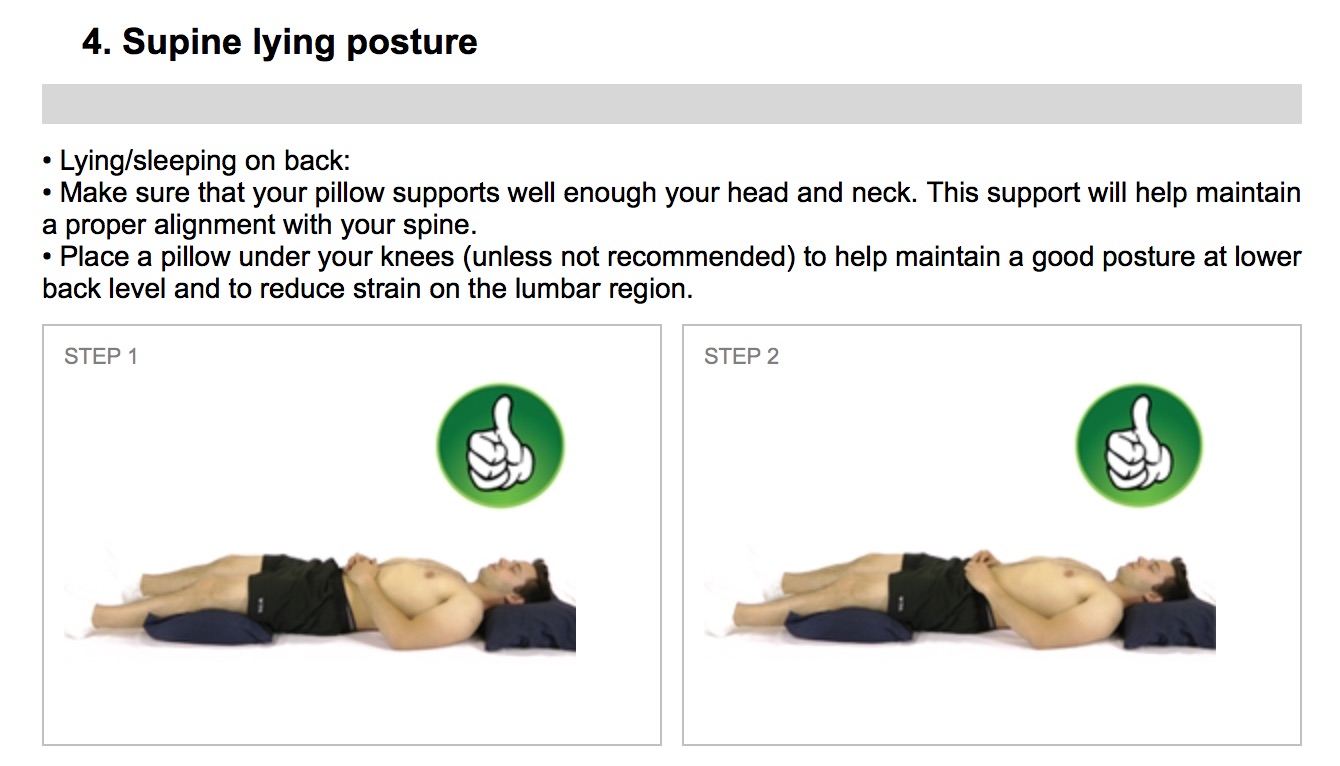
The other recommended sleep position is lying on the back, with 1 or 2 pillows under the knees to reduce the arch in the lower back. Lying flat on the back with the legs flat tends to cause an arch in the lower back, which can cause stress on the facet joints of the lower back and shortening of the muscles in the low back.
So we have compiled this quick visual guide of sleeping positions.
Sleeping on the tummy can strain the neck and the lower back
Sleeping on the side with a cushion between the knees is ideal
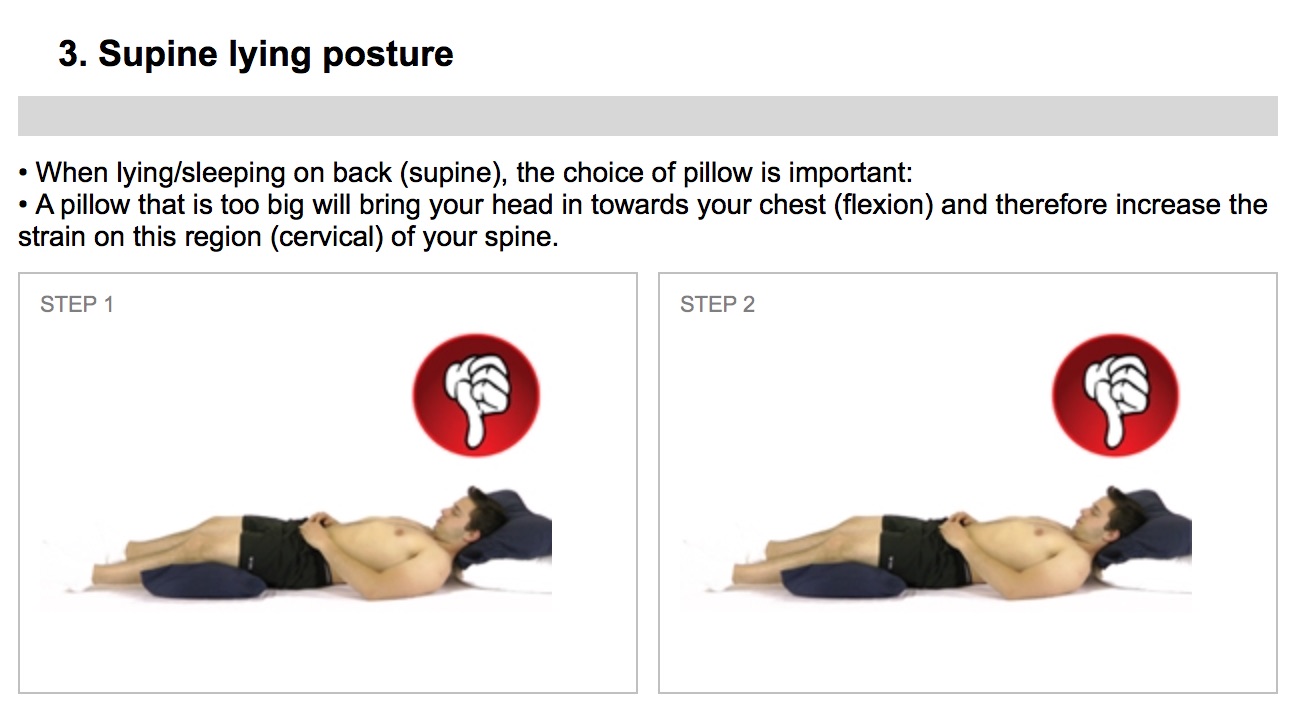
Too many pillows under the head
BOOST PHYSIO is a leading private physiotherapy practice with high street clinics across North West London. We have 4 branches in the following areas: . Branches of our physiotherapy practice are in Cricklewood NW2, Hampstead NW3, Hendon NW4 and East Finchley N2.
Our private physiotherapy clinics treat patients from all over North West London and North London. We provide same day physiotherapy treatment for sports injuries, neck and back pain. Appointments are available 8am to 9pm and we even have Saturday and Sunday appointments available.
Patients come for physiotherapy from the following areas: Hendon NW4, Mill Hill NW7, Cricklewood NW2, Hampstead NW3, Kilburn NW6, Queens Park, Finchley Road, Golders Green NW11, Swiss Cottage and Willesden Green NW10. Fortis Green, Muswell Hill, Highgate N6. East Finchley N2.
If you do have nay issues that need attention please book an appointment at one of our 4 High Street Physiotherapy clinics.
Are your legs ski ready? Our 5 key exercises to help you prepare.
As the ski season approaches you should be thinking about preparing your body for the demands that skiing places upon it. Skiing is great a sport enjoyed by many people, however, it can place a lot of stress and strain on your muscles and joints- particularly the knees and legs! If you are planning a ski trip this winter, now is the time to start preparing.

We all enjoy the thrill of speeding down black runs and bouncing over moguls, but what we don’t appreciate is that burning feeling in the legs after a long day on the slopes! This is where doing preparatory work strengthening the leg and hip muscles can help ensure you make the most of each day on the slopes injury free and trouble free.

Our 5 Key ski prep exercises
By strengthening your “ski specific” quadriceps, hip and core muscles and by practicing exercises to improve your balance and ski posture, you will create a more efficient skiing technique in order to reduce the risk of injury and muscle aches, ultimately making your skiing trip more enjoyable.
If you need any help getting ready for ski season, or have any niggling injuries, now is the time to sort them out, before your ski holiday. Don’t let a niggly knee spoil your holiday.
Call us now on 020 7794 9078 and one of our expert physiotherapists will help you get sorted!
NEVER do these 2 exercises in the gym!
Unless you want to risk potentially serious injuries, I believe you should never do the following 2 exercises. It still amazes me how many people I see doing these exercises in the gym. All exercises have benefits, but they all carry a potential for injury. The following 2 exercises in my view are potentially too risky from an injury point of view.
1) DEAD LIFTS: Dead Lifts place enormous stress and strain on the lumbar spine

and the discs between each of the vertebra. By doing Dead Lifts one stands a great chance of injuring the lower back region, in particular a nasty injury to the intervertebral discs.
There are many other, safer exercises that can be done to exercise the desired muscles, without injuring oneself. Bending forward from the waist to pick things up from the ground is particularly stressful on the lumbar discs and soft-tissues around the area, this is why most people know that one should not bend down from the waist to pick things up. It is therefore surprising to see so many people doing dead lifts in the gym.
2) UPRIGHT ROWS: This is an exercise that is often done to strengthen the shoulder muscles and the trapezius muscles (those muscles that lie between your shoulders and your neck).

Unfortunately this exercise often leads to a pinching of the supraspinatus tendon, part of the rotator cuff muscles. This condition is often called impingement syndrome and causes irritation and swelling of the tendon and can lead to supraspinatus tendinitis.
In cases of chronic pinching of the supraspinatus tendon in the shoulder, the tendon can become frayed and torn. In severe cases this can require surgery to repair the torn tissue. In addition, most people do not need their trapezius muscles strengthened and built up, as it is usually tight and overworked already.
The risk-reward ratio for this exercise shows that the risks of injury outweigh the potential benefits and in our view this exercise should always be avoided.
If you are having shoulder pain or trouble, you should come and be examined by one of our expert physiotherapists who will be able to treat and advise you to ensure a speedy recovery.
Information Links
Physiotherapy Organisatons
The Chartered Society of Physiotherapy (CSP):
http://www.csp.org.uk
Health Professions Council (HPC):
http://www.hpc-uk.org/
Health Professions Council Check (HPC Check):
http://www.hpccheck.org
Acupuncture Association of Chartered Physiotherapists (AACP):
http://www.aacp.uk.com
Manipulation Association of Chartered Physiotherapy (MACP):
http://www.macpweb.org
PhysioFirst:
http://www.physiofirst.org.uk
Association of Chartered Physiotherapists Interested in Neurology (ACPIN):
http://www.acpin.net
Companies*
North London Neuro Physio:
www.northlondonneurophysio.com
Pilates for One, Two or Three:
0208 381 4061 (Fran Michelman)
Align Pilates Studio:
079 4274 2232 (Katherine Brown)
Services*
Fleet Cars (local mini cab service):
0207 485 7777
Swiss Cottage Cars (local mini cab service):
0207 431 2700
* The above resources are operated by parties other than The Hampstead Physiotherapy Practice. Although we take care to ensure the above resources and links are accurate and reputable, we cannot guarantee this. The inclusion of the above resources are for your convenience only and does not imply any reliability or endorsement of the content of such companies from The Hampstead Physiotherapy Practice.